What Is Acute Pancreatitis?
The pancreas is a boomerang-shaped organ within the abdominal cavity. It performs several essential functions. Most importantly, it produces digestive enzymes that allow dogs to break down fats, proteins, and carbohydrates. Acute pancreatitis develops when the pancreas becomes suddenly inflamed.
Normally, digestive enzymes activate in the intestinal tract. However, during acute pancreatitis, these enzymes activate prematurely inside the pancreas. Consequently, they trigger intense local inflammation. In mild cases, inflammation stays localized and reversible. In contrast, severe cases allow inflammatory mediators to enter systemic circulation. As a result, distant organs such as the lungs, kidneys, heart, and coagulation system suffer secondary injury. Therefore, clinicians should view acute pancreatitis as a systemic inflammatory disease, not merely a gastrointestinal disorder.
Although pathologists classify pancreatitis as acute or chronic, clinicians cannot reliably distinguish these forms without biopsy. Thus, the preferred clinical term is acute-onset pancreatitis, which reflects sudden onset or worsening of clinical signs regardless of underlying chronic changes.
Risk Factors for Acute Pancreatitis in Dogs
Acute pancreatitis arises from multiple interacting factors. Although many cases remain idiopathic, several well-established risks increase susceptibility.
Breed and Genetic Risk
Dogs at increased risk include:
- Miniature Schnauzers
- Dachshunds
- Poodles
- Cocker Spaniels
- Fox Terriers
- Laikas
- Alaskan Malamutes
Importantly, Miniature Schnauzers carry a high prevalence of familial hypertriglyceridemia, a genetic disorder that elevates serum triglyceride concentrations. Moreover, evidence shows that hypertriglyceridemia, not hypercholesterolemia, drives metabolic risk.
Metabolic and Systemic Disorders
- Diabetes mellitus
- Hypertriglyceridemia
- Hypercalcemia
- Chronic kidney disease
- Neoplasia
- Congestive heart failure
- Autoimmune disease
- Inflammatory bowel disease
Body Condition and Age
- Iving with overweight or obesity
- Age greater than 7 years
Dietary Factors
- Ingestion of fatty meals
- Table scraps
- Trash or unfamiliar foods
Notably, dietary indiscretion remains one of the most frequently reported historical triggers.
Medications and Toxins
Medications most often associated with pancreatitis include:
- Potassium bromide
- Phenobarbital
- Azathioprine
- L-asparaginase
Although drug-induced pancreatitis occurs infrequently, any medication may act as an idiosyncratic trigger. Therefore, clinicians should obtain a careful medication history, especially in dogs with prior pancreatic inflammation.
Clinical Signs of Acute Pancreatitis in Dogs
Dogs display a broad spectrum of disease severity. Some experience mild, self-limiting illness. Others, however, develop severe, life-threatening disease.
Common clinical signs include:
- Dehydration
- Loss of appetite
- Vomiting
- Weakness or lethargy
- Abdominal discomfort
- Diarrhea
- Fever
- Jaundice or icterus
Importantly, clinicians often underestimate abdominal pain. Dogs may not assume a classic prayer posture. Instead, tachycardia, tachypnea, restlessness, trembling, or reluctance to move frequently indicate significant discomfort.
Potential Complications
Severe acute pancreatitis may progress rapidly. Consequently, affected dogs can develop:
- Systemic inflammatory response syndrome
- Acute respiratory distress syndrome
- Disseminated intravascular coagulation
- Acute kidney injury
- Cardiac arrhythmias or myocarditis
- Pleural effusion or pulmonary edema
Additionally, transient hyperglycemia or diabetic ketoacidosis may occur due to insulin resistance or beta-cell dysfunction. Fortunately, many dogs regain normal glucose regulation as inflammation resolves.
How Is Acute Pancreatitis Diagnosed in Dogs?
Pancreatic biopsy remains the diagnostic gold standard. However, most dogs with suspected acute pancreatitis cannot safely undergo anesthesia. Therefore, clinicians diagnose the disease by integrating clinical signs, laboratory data, and imaging findings.
Laboratory Testing
- Complete blood count
- Serum biochemical profile
- Urinalysis
Pancreas-Specific Tests
Measurement of serum pancreatic lipase provides the most sensitive and specific clinicopathologic support for diagnosing acute-onset pancreatitis in dogs.
Common assays include:
- SPEC cPL™
- SNAP cPL™
- PrecisionPSL™
Diagnostic Imaging
- Abdominal radiographs: Clinicians use radiographs to exclude alternative causes of gastrointestinal signs. However, radiographs rarely confirm pancreatitis.
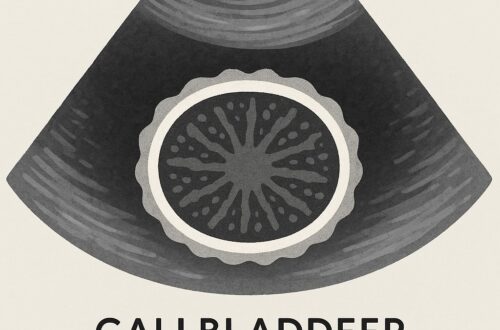
- Abdominal ultrasonography: When performed by an experienced ultrasonographer, ultrasound more reliably identifies pancreatic inflammation, peripancreatic fat changes, bile duct obstruction, and complications.
Early collaboration with specialists improves diagnostic efficiency. Moreover, it often reduces unnecessary testing.
Treatment of Acute Pancreatitis in Dogs
No antidote exists for acute pancreatitis. Instead, treatment aims to prevent disease progression, limit systemic inflammation, and manage complications.
Core Treatment Goals
- Identify and correct underlying predisposing factors when possible
- Deliver aggressive, evidence-based supportive care
Fluid Therapy
Fluid therapy plays a central role. However, indiscriminate aggressive resuscitation increases the risk of fluid overload without improving outcomes. Consequently, current evidence supports goal-directed crystalloid therapy with a balanced electrolyte solution. They should reassess hydration status, perfusion, and ongoing losses frequently.
Analgesia
Clinicians should assume pain in all dogs with pancreatitis.
- Full mu-opioids such as fentanyl or methadone often provide necessary analgesia
- Clinicians should avoid nonsteroidal anti-inflammatory drugs because of gastrointestinal and renal risks
- Opioid-sparing strategies, including lidocaine or ketamine constant-rate infusions, may reduce ileus and shorten hospitalization
Importantly, teams should reassess pain scores every 2 to 4 hours and adjust therapy promptly.
Antiemetic Therapy
Effective control of vomiting improves comfort and facilitates early nutrition.
- Maropitant serves as a first-line antiemetic
- Ondansetron adds antinausea benefit through a complementary mechanism
- Metoclopramide should not serve as a primary antiemetic
Nutritional Support
Prolonged fasting worsens outcomes. Therefore, clinicians should initiate nutrition early whenever possible.
Early enteral nutrition:
- Preserves intestinal barrier function
- Reduces bacterial translocation
- Improves clinical outcomes
If voluntary intake does not resume within 24-36 hours, clinicians should initiate assisted enteral nutrition using a nasoesophageal or nasogastric feeding tube. In contrast, force or coax feeding promotes food aversion and delays recovery.
Antibiotics
Routine antibiotic use does not improve outcomes. Thus, clinicians should reserve antibiotics for dogs with clear evidence of:
- Aspiration pneumonia
- Bacterial translocation
- Documented infection
Anti-Inflammatory Therapy
A targeted therapy, fuzapladib sodium, inhibits neutrophil extravasation and improves clinical activity scores in dogs with acute pancreatitis. Notably, it represents the first disease-specific pharmacologic therapy and holds FDA conditional approval in the United States.
Corticosteroids remain controversial. Although limited retrospective data suggest potential benefit in select cases, clinicians need additional prospective studies before routine use.
Prognosis
Most dogs with mild to moderate acute pancreatitis recover with appropriate supportive care. However, dogs with severe disease face a guarded prognosis, particularly when systemic inflammation, respiratory compromise, coagulation abnormalities, or acute kidney injury develop. Therefore, early referral to specialists markedly improves the likelihood of a favorable outcome.
Key Take-Home Messages
Acute pancreatitis in dogs represents a complex, systemic inflammatory disease with variable severity. Early recognition, integrated diagnostics, evidence-based supportive care, prompt nutritional support, and thoughtful use of emerging therapies collectively improve survival and long-term quality of life.